
Case-Report | DOI: https://doi.org/10.31579/2578-8868/115
Department of Neurological surgery, University of Pittsburgh School of Medicine UPMC Hamot, Erie, PA USA
*Corresponding Author: Salem El-Zuway, Department of Neurological surgery, University of Pittsburgh School of Medicine UPMC Hamot, Erie, PA USA
Citation: Salem E. Zuway., Bellotte J. (2020) Lumbar Spinal Hemorrhagic Intradural Meningioma Misdiagnosed as Acute Lumbar Disc Radiculopathy: Case Report. J. Neuroscience and Neurological Surgery. 6(2); DOI:10.31579/2578-8868/115
Copyright: © 2020 Salem El-Zuway, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any Medium, provided the original author and source are credited.
Received: 31 January 2020 | Accepted: 12 February 2020 | Published: 17 February 2020
Keywords: spinal; meningioma; intradural; subdural; subarachnoid; hemorrhage
BACKGROUND:
Spinal meningiomas are slow growing benign tumors arising from arachnoid cap cells throughout the spinal meninges. Spontaneous bleeding is extremely uncommon and scarcely reported in literature.
CASE PRESENTATION:
We present an 81-year-old male patient who presented to the emergency department with a sudden onset of severe thoracolumbar back pain, radiating to both legs with weakness and paresthesia. Thoraco-lumbar spine MRI with gadolinium depicted an L1-L2 intradural spinal tumorous mass with intraspinal hemorrhage. He underwent an urgent laminectomy for tumor resection and hematoma evacuation. Histopathology confirmed the diagnosis of meningioma WHO grade I.
CONCLUSION:
Spinal meningiomas presenting primarily with hemorrhage are scarcely reported in literature. To our knowledge, two cases have been reported. A high index of suspicious is crucial as a timely surgical intervention significantly influence the degree neurological recovery.
Limits:
# of abstract words - 131
# of text words – 1,148
# of references – 6
# of tables/figures - 5
# of videos – 0
Spinal meningiomas are slow growing, indolent relatively uncommon tumors. Approximately about 6% are located in the thoracolumbar spine region and comprise of about 1.2% of meningiomas of the central nervous system [1]. Spontaneous intraspinal hemorrhage from meningiomas often presents as an epidural as the most prevalent form, nevertheless the clinical distinction from subdural or subarachnoid can be quite challenging [2]. Additionally, the specifics governing each individual form of presentation depend on the tumor location. Although variable number of risk factors linked to pathogenesis of the neoplasm hemorrhagic diathesis are reported, nonetheless, there is still paucity of well documented cases in literature. Such factors include coagulation disorders, spine trauma and spinal injections [3].
We report a rare case of an 81-year old male patient with a newly diagnosed upper lumbar spine intradural extramedullary meningioma presenting primarily with intraspinal subarachnoid hemorrhage after out of proportion physical exertion.
Case report:
An 81-year-old male patient had a history of hypertension & hypothyroidism presented to the emergency department with a sudden onset and progressive severe low back pain started four days prior to presentation when he attempted to climb up on a chair to change a light bulb. Initially he felt a sudden of intense stabbing low back pain radiating to both legs. He went to his primary care physician who initially diagnosed him as a case of acute lumbar disc herniation managed him with outpatient pain control. A few days later the intensity of pain has progressively gotten worse and subsequently developed progressive bilateral leg weakness and urinary retention. He went to the emergency department and cauda equina syndrome was diagnosed and Foley catheter was indwelled and an urgent MRI spine was ordered which depicted evidence of an L1-L2 intradural spinal mass and urgent neurosurgical consultation was sought. He was complaining of weakness in both legs worse on the right side and is associated with numbness and tingling sensation in both feet. He denied any history nausea, vomiting, injury, fall, saddle anesthesia or bowel incontinence on admission. No history of anti-platelets or anti-coagulation therapy intake.
Right lower extremity exam: Hip flexion 2/5, foot dorsiflexion 1/5, Extensor hallucis longus (EHL) 1/5, plantar flexion 1/5. Left lower extremity exam: hip flexion 3/5, knee extension 4/5, foot dorsiflexion 3/5, EHL 4/5, plantarflexion 4/5. Sensation to light touch and pinprick was markedly reduce in both extremities in all dermatomes but intact perineal sensation and rectal tone. Absent deep tendon reflexes in both knees and ankles. Negative Babinski’s and clonus signs bilaterally. Upper extremity examination was unremarkable.
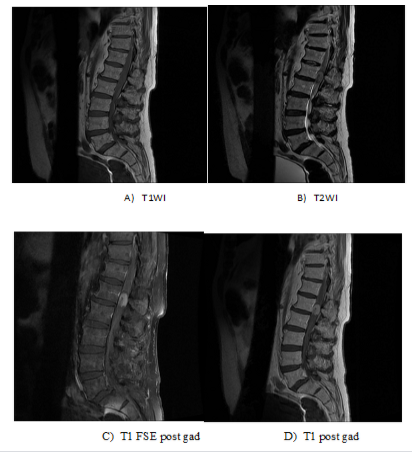
Neuro imaging:
MRI of lumbosacral spine with and without contrast (Figure 1. A-D) depicted an intradural extramedullary mass lesion L1-L2 region level. The mass is about 2.5cm x 1.3cm and is hypointense on T1 and mixed hyper- and isointensity on T2-weighted images and avidly enhances with contrast administration with central non-enhancing heterogenous core.
Surgical intervention:
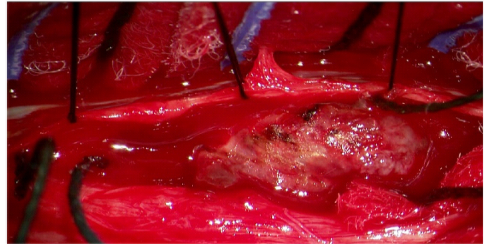
The patient underwent an urgent L1-L2 laminectomy via midline approach using intraoperative neurophysiological monitoring of somatosensory evoked potentials (SSEPs). Tumor location was further confirmed using intraoperative Realtime sonogram. The thecal sac was quite swollen and once the dura was opened, immediately encountered a gush of both acute and altered blood with multiple clots above and below the tumorous lesion (Figure 2).
The tumor-dural attachment was to the right lateral wall. The conus medullaris and cauda equina nerves were severely compressed by the hemorrhagic mass and acute blood components. Internal debulking was initiated to avoid any pressure on the conus medullaris or the cauda equina nerves and a gross total resection was achieved under microscopic magnification in a piecemeal fashion under meticulous microdissection with a low voltage irrigating diathermy hemostasis and copious amounts of irrigation with saline, the dura was closed in a watertight fashion. The patient tolerated the procedure well and the immediate postoperative period was remarkable for a dramatic pain relief. Throughout the course of follow-up the patient achieved significant improvement in motor and sensory functions and bladder sensation and regained full bladder function and rehabilitation program followed.
Pathology report:
The pathology report was suggestive of meningioma WHO grade I with the gross picture of multiple fragments of hemorrhagic and tan-white soft tissue pieces. On the microscopic level it depicted tumor cells which demonstrated vimentin positive, EMA positive (weak staining), S100 positive, Progestogen Receptor positive (nuclear staining), GFAP negative (0%). The Ki-67 proliferation index is 1%.
Discussion:
The clinical presentation of this patient to the primary care practice was definitely challenging as the classic sudden onset of low back pain with radicular lower extremities pain in the setting of vigorous physical exertion, the pretest probabilities will be on the high side of a lumbar disc prolapse rather than of a neoplastic nature. Spinal meningiomas are rare, generally benign intradural extramedullary tumors that originate from arachnoid cap cells along the entire spinal dura and they represent roughly around 25% of primary spinal cord tumors. These are mainly predominant in females (80%). They usually present depending on their location in the spine with either myelopathy or mixed myeloradiculopathy. Spontaneous hemorrhage from spinal meningiomas is quite uncommon and seldomly reported [4]. To our knowledge, two cases have been described in literature, one of them is nonspontaneous due to iatrogenic lumbar puncture
[3, 5]. These mostly present as extratumoral and subarachnoid hemorrhage. Less likely as subdural or intratumoral bleed [3]. Although the classic description of a sudden onset of severe back pain associated with progressive paraplegia, myelopathy, radiculopathy or mixed sphincter dysfunction has been described in patients harboring a spinal meningioma; to our knowledge, spontaneous nontraumatic non-coagulopathic neoplastic hemorrhage due to over stretching or strenuous physical exertion has not been previously reported especially with low grade (WHO grade I) with very low proliferation index (Ki-67 1%). MRI with contrast is the gold standard for working diagnosis. The exact pathophysiology of tumorous bleeding has not yet identified but it is believed to be related to extratumorous microvascular shearing injury [4].
Here we present in a case with a non-traumatic spontaneous hemorrhage within a conus medullaris spinal meningioma in a non-coagulopathic patient with no known risk factors. The bleeding was an extratumoral subarachnoid hemorrhage with blood clots above and below the main bulk of the neoplasm. The exact pathophysiological mechanism of this spontaneous bleeding is not clearly understood but likely related to mechanical injury by microvascular shearing of the peri-neoplastic microvasculature during the vigorous over-stretching maneuvers that the patient was undergoing with possible venous congestion of small fragile peri-tumorous vessels leading to hemodynamic changes and subsequent rupture. Extensive literature review did not clearly divulge a spontaneous burst of spinal tumors in a quiescent setting.
This is obviously a neurosurgical emergency and early detection mandates a prompt operative intervention could significantly impact and substantially lower the risk of functional impairment and long-term disability. The extent of neurological deficit encountered at the time of emergency department presentation is a quite crucial predictor on the degree of functional recovery following a successful gross total resection of the tumor. Haegelen reported in his retrospective series of 33 patients with severe preoperative neurological deficit about 2/3 of them achieved total recovery [6]. so if the high index of suspicious in patients with no known risk factors with this classic presentation, early surgical intervention is high indicated for a favorable neurological functional outcome.
Future work:
These tumors are quiet scarcely reported in literature and due to the fact of paucity of information on a larger scale population study, a pooled data analysis of case reports is a future work plan and can provide more information about the nature and outcome of these tumor behaviors.
Conclusion:
Spinal meningioma presenting with spontaneous hemorrhage is very rare. A high index of suspicion in patients with no known risk factors who presents with sudden onset of severe back pain, progressive leg weakness or sphincter dysfunction, warrants immediate investigation with MRI evidence of a spinal warrants a prompt surgical intervention as it is clearly shown to correlate with functional recovery.
Financial: No financial disclosures or conflict of interest
Paper not previously presented or published either in part or in full
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
